John is too distraught and anxious. He is incapable of taking out the trash, sort out his laundry, even decide what to wear. Frantically, the only time he picks up the phone is to call his cousin and let her, miles away, guide him on how to do the mundane activities he was once able to do. Plagued by the uncertainty of his future, his stagnation is fueled by the sorrow of his heartbreak.
The psychiatrist deems John too unstable to go back to his empty apartment, let alone, function in society. John is committed to the inpatient unit to stabilize. His cousin is very pleased with this decision.
John is grieving the loss of his wife and eleven year old daughter to the perils of divorce. He was let go from his employment, he cannot afford his condo, and for the first time he has to care for self.
John’s case is just one example of how the prevalent Western medical model approach deems what is functional or not societal. Luckily, John went to the Emergency Room and was voluntarily admitted. Other patients are not so docile when they are brought into the ER. Repressed emotional, mental, physical, and spiritual pain detonated in the community is received with hostility and ridicule, not only in the community, but, also in the “safe” haven of the hospital setting where pain and suffering is alleviated with medication and subjugation.
One such depiction of the detached medicalization of deviant behavior is illustrated in a documentary on New York City’s Bellevue’s Psychiatric ER. The following is a screen shot of the two attending psychiatrists discussing the incoming patient’s admission to the ER. 
In this mis-en-scene, Dr. Rives (on the left), and Dr. Fernandez-Milo, Psychiatric ER Associate Director (on the right) discuss what brought a male patient to the ER. The discussion takes place in the ER corridor, at the head of the patient’s stretcher while the hand-held camera pans to the POV shot of the patient restrained to a stretcher, wearing a protective spit shield while screaming, yelling, flailing, and contorting. In this medium shot both doctors are seen laughing as they share the presenting problem and patient’s behavior as he attempted to burglarize a home. Dr. Fernandez-Milo laughs as he states that when the police arrived the patient “started his dramatics” as he was being cuffed. It is known that humor is a usual defense mechanism to deal with a traumatic event. However, in this case the medical model’s phlegmatic, indifferent and detached protocol imparts shaming and even ridiculing of the deviant’s behavior. To subdue the deleterious behavior, an injection of Haldol is administered in order to silence the patient as he is still handcuffed to the stretcher. .
Similarly, the hand-held camera pans to another POV shot of Dr. Rosenberg (on the right of the screen) laughing as the police officer reports that the patient also attempted to bite someone and is facing legal charges.
How does the pained person feel when his fate is in the hands of detachment and subjugation?
It is said that the strength of the medical model is in its objectivity and medication protocol which creates almost immediate relief (McLeod, 2008). However, within its reductionist, biological, and detached paradigm, the medical model contradicts the Hippocratic oath of “first, do no harm” (Shah and Mountain, 2007 pp. 375). One section of the Hippocratic oath states that,
“I will remember that there is art to medicine as well as science, and that warmth, sympathy, and understanding may outweigh the surgeon’s knife or the chemist’s drug…”(MedicineNet.com).
If compassion, sympathy, and empathy towards the pained person comes first before the utilization of extremely harmful, humiliating, and controlling practices, the Hippocratic oath is fulfilled. As observed in the above screenshots, the physicians do not present as objective or compassionate to the patient’s disposition nor pain. Detached either through humor, defense mechanisms, judgement and/or status, the pained person’s fate is in their control. The communal judgment, labeling and banishment through hospitalization is contrary to the Hippocratic oath. It is also a reenactment of past historical practices proven to be against a person’s civil liberties, as well as, ineffective and cruel. If the clinician, social worker, doctor, or nurse, can find compassion through their own humanity, perhaps the Hippocratic oath would be upheld and practiced. Yet, compassion and empathy is felt when an individual is present and emphatically mindful of another’s suffering through their own healing and empowerment.
The following screen shot portrays how two individuals in shared isolated pain joining through compassion and empathy.
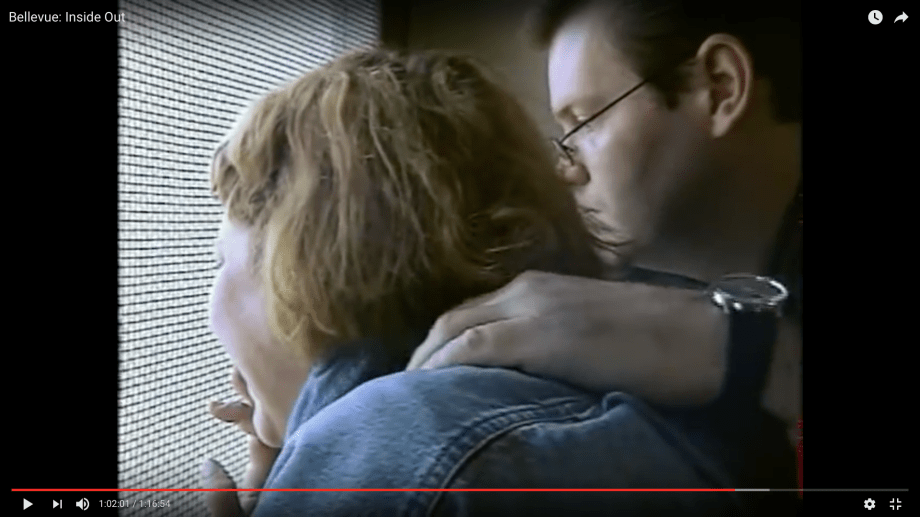
This close up shot with a hand-held camera depicts two patients by a window. Both were released from the hospital’s court. The male patient is a voluntary patient who presented upon admission with suicidal ideation due to marital stress. This patient has no prior psychiatric history. He is diagnosed with bipolar disorder with psychotic features, a danger to self, and others. Prior to the hospitalization, the patient’s only “crime” was to watch pornography and masturbate six hours a day hindering any other productivity, as well as straining his marital relationship. In court he presents as an articulate, assertive, and respectful person who is able to convince the judge that he does not need or want medication. Based on this presentation, the judge concedes but still recommends further treatment. The patient declines and signs himself out of the hospital AMA (Against Medical Advise).
The female patient’s fate is very different. Diagnosed with schizophrenia and possessing legal charges, she is court mandated to be confined in the hospital until the system deems her suitable to return to the community. In other words, judged a menace to the society, she is medicated, numbed, and excommunicated from the community.
Without contact with the outside world for some time, this close up shot depicts compassion and empathy between two individuals who identify and commune in shared pain. The pan shot follows both patients down the hospital corridor as the male patient benevolently guides her to a barred window where she can get a glimmer of sunshine and get a glimpse of the outside world.
As it can be seen, she is desperate in her hopelessness and helplessness. Is this depiction of patient treatment, one of curing or harming? Based on this particular scene and many others in the documentary, the end result of treatment seems to be more of harm, if not punishment. If both patients are considered a danger to self and others, the biased discharge decision may be based on socioeconomic status and potential productivity. In observing both patients, the male patient is wearing a suit, perhaps, indicating that he can hold employment or had one in the past. While, in contrast, the female patient, appearing disheveled, labeled and with a history of hospitalizations and legal charges is the one deemed to be a menace to society. She is hospitalized, without a chance to breathe the outside air, until the judge of the people rules her fit to rejoin her marginalized community. Hospitalization did not help either patients. Both were labeled, medicated, and confined.
Shifting Perspectives from Biological Reductionism to Compassionate Presence in the Face of Trauma
As evidenced in the above screenshots, compassion and empathy for the suffering of another can be absent in the utilization of the medical/scientific model to deal with trauma. On one hand, it is incomprehensible that an injection of Haldol or isolation can deal with the origin of the trauma. Yet, on the other hand, the healing presence of another may assist in relieving the pain and get to that origin of trauma. The psychic pain manifested through acting out behaviors can be eased through the calming presence of an empowered other. Perhaps the acute distress of a pained person can be mitigated through the administration of a calming agent in a respectful and calming demeanor in conjunction with psychotherapeutic treatment other than what is portrayed in the documentary.
What can the State of Compassionate Presence Look Like in a Therapeutic Encounter?

The above screenshot and the one that follows focus on a psychotherapeutic demonstration between the Phenomenological and Existential psychotherapist, Dr. Alfried Langle and his volunteer client, Bruce, a family therapist from Vancouver. This phenomenological encounter and demonstration took place in the campus of the University of British Columbia on October 18, 2007.
Notice the eye contact between Dr. Langle (on the left) and Bruce as he recounts his sense of loneliness and addictions as he grew up with his detached adoptive mother. Dr. Langle’s body language and facial expression conveys understanding as Bruce conveys being heard and understood. It is in this abstract state of presence that Bruce to can contemplate and de-escalate. 
During this medium shot, the audience’s perspective of the encounter is transmitted through the artistic, open-minded, healing interconnection between the two protagonists. Through Dr. Langle’s gentle, kind, respectful, yet inquisitive presence, Bruce is able to work through his psychic pain and overt aggression by finding his inner gifts and strength.
